
Prader-Willi syndrome overview
Last updated Sept. 18, 2025, by Lindsey Shapiro, PhD
 Fact-checked by Marta Figueiredo, PhD
Fact-checked by Marta Figueiredo, PhD
Prader-Willi syndrome (PWS) is a rare condition characterized by a wide range of symptoms, typically including insatiable hunger, slow growth, intellectual disability, and behavioral issues, that are caused by genetic abnormalities affecting chromosome 15.
While there is no cure for this genetic disorder, a prompt diagnosis and an early start to treatment can make living with PWS easier.
Although the disease itself is not life-threatening, complications related to extreme overeating and obesity can substantially impact PWS life expectancy. However, if diet is well controlled and obesity is avoided, people with PWS can have a relatively normal lifespan.
Prader-Willi syndrome causes
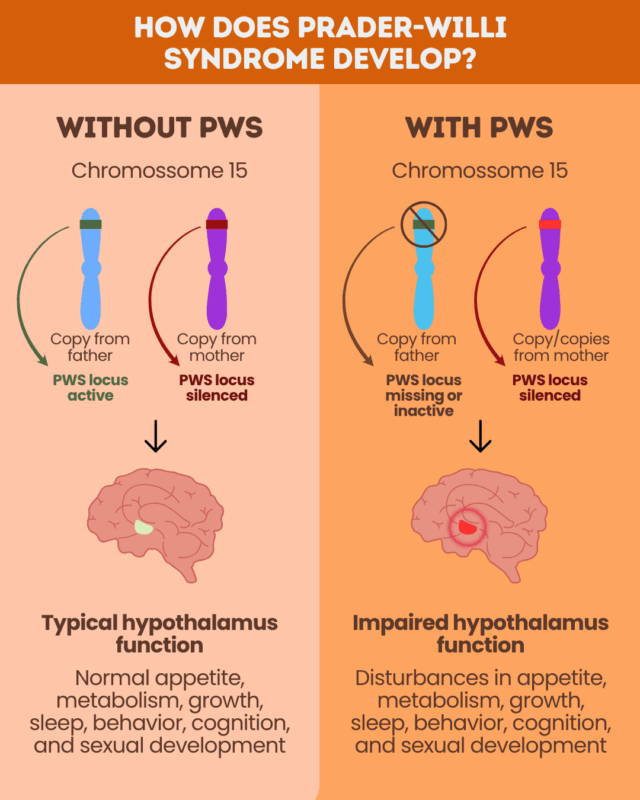
The underlying PWS causes are genetic defects that result in the loss or inactivation of paternally inherited genes on a particular section of chromosome 15, called the PWS locus. This is thought to affect the function of the hypothalamus, a brain region that controls hunger and other bodily processes.
Through a natural process called genetic imprinting, the paternal genes on the PWS locus are normally active, while those inherited from the mother are silenced. There are three main defects that can cause the loss or inactivation of paternal PWS locus genes:
- a chromosome 15 deletion, where paternally inherited genes in the PWS locus are missing
- maternal uniparental disomy, where two copies of chromosome 15 are inherited from the mother and none from the father
- imprinting defects, where the paternal PWS locus genes are mistakenly silenced
Prader-Willi syndrome symptoms
There is a wide range of possible PWS symptoms, which can vary between individuals and by age. Some of the most common ones are:
- poor muscle tone, called hypotonia, and feeding difficulties in infancy
- short stature and small hands or feet
- insatiable appetite, known as hyperphagia, starting in childhood, and leading to obesity
- motor developmental delay
- learning and speech difficulties
- sleep disturbances
- mood and behavioral problems, like temper outbursts and stubbornness
- underdeveloped sex organs, delayed puberty, and infertility
Other possible symptoms include:
- distinct facial features, including almond-shaped eyes, a narrow forehead, and a downturned mouth
- thick saliva and tooth issues
- orthopedic issues such as scoliosis, an abnormal spine curvature
- unusually light skin, hair, and eyes
- body temperature regulation issues
- crossed eyes
- reduced sensitivity to pain
Prader-Willi syndrome diagnosis
PWS is first suspected when an infant, child, or teenager shows age-specific clinical features of the disease. Genetic testing is then performed to establish a PWS diagnosis and identify the type of genetic defect.
A DNA methylation analysis is typically the first genetic test, as it effectively identifies about 99% of PWS cases by detecting missing or silenced genes on the paternally inherited PWS locus. Because it cannot typically distinguish between the major types of PWS-causing genetic abnormalities, however, other genetic tests are then run to determine the specific defect.
Prader-Willi syndrome treatment
PWS treatment is focused on easing symptoms and improving life quality. Treatment strategies depend on the patient’s age and symptoms, but generally involve a multidisciplinary team of specialists.
Treatment for PWS may involve:
- Ensuring adequate nutrition: Due to weak sucking, babies with PWS may need a feeding tube or specialized formulas to promote weight gain in their first years.
- Growth hormone therapy: Treatment to combat the deficient levels of growth hormone seen in most PWS patients is typically started early in life. It helps improve growth and metabolism.
- Weight management: Children and adults with PWS need strict food control and a low-calorie diet to prevent hyperphagia-related obesity. Individuals ages 4 and older may be prescribed Vykat XR (diazoxide choline), a daily oral therapy approved in the U.S. to ease PWS-related hyperphagia.
- Sex hormone replacement therapy: Due to the PWS-associated impaired production of sex hormones, this type of therapy is commonly started around the time of puberty to promote normal sexual development and bone health. Surgery may be needed for undescended testicles in boys.
- Sleep management: Medications, ventilation support, or other interventions can help ease PWS-related sleep issues such as sleep apnea or excessive daytime sleepiness.
- Behavior management: Behavioral therapy, sometimes used with antidepressant medications, can help control the behavioral symptoms of PWS.
- Physical, occupational, and speech therapy: These interventions can be used to improve motor and speech skills and help with daily life activities.
Prader-Willi Syndrome News is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.